Introduction and explanation for the purpose of a “Paper Trail”
These are some of the published journal articles with which I have been involved during the past 57 years since 1963. In many entries there is a story or information relating to the publication which does not appear in the text. There is some information relating to the many friends and colleagues involved as co-authors or main authors and some information about their lives. I found this “where are they now” aspect particularly interesting; this was only possible using the modern media facilities. Even at this stage I had some surprises!
The majority of the publications mentioned are listed on PubMed and the PMID number is included with most of the references which, if entered into PubMed, will take you to the original full abstract. In some there is a direct link to the PubMed abstract. If “FREE is mentioned, a free full copy can be accessed from the PubMed entry. As my life and my family, until they went their own ways, were influenced by my professional activities it seemed important to include them at various stages. Indeed they have been a source of joy and great support overt the years.
The “Paper Trail History” slightly edited and updated in 2026. I have added comments on the subsequent significance of the publications and follow-up of some of the reports and the people described.
How did I enter the Paper Trail?
The first publication in the paper trail was from 1963 when I was a Registrar Tutor in Professor Stuart Craig’s University Department of Paediatrics and Child Health in Leeds. When finished my 2 years National Service with the RAMC in 1959 (described in more detail on this website (.jimlittlewwod.com “1957-1959 Royal Army Medical Corps”) and after a few months as a locum casualty officer at the Leeds Public Dispensary, I was keen to pursue a career in surgery and very fortunate to obtain one of the three excellent casualty officer posts with the legendary Mr Maurice (“Father”) Ellis at the Leeds General Infirmary. His accomplishments are listed on the Blue Plaque eventually erected outside the Leeds General Infirmary.

After working with Mr Ellis in the LGI Accident and Emergency Department for about four months (described in detail on www.jimlittlewood.com. “Sixties from Casualty Officer to Paediatrics”), I was approached by Dr George Lewis, a Lecturer in Paediatrics with Professor Stuart Craig in the University Department of Paediatrics and Child Health. I knew both George and Professor Craig from my time as the Paediatric House Physician in 1956. George suggested we meet the following evening for a drink at the Tunbridge, the pub behind the Infirmary frequented by the medical staff, as there was a matter the Professor had asked him to discuss with me. We duly met in the Tunbridge that evening as arranged and George asked if I would be interested in returning to paediatrics!

I had been the paediatric house physician for six months with Prof. Craig and Dr. Eric Allibone at the LGI after I qualified in 1956 and certainly had enjoyed the job. Also, I had done the paediatric locum in the LGI for two periods of two weeks when a medical student. Even so, at this stage, I had no intention of following paediatrics as a career.and had never seriously considered the possibility.

At our meeting George indicated Prof. Craig was impressed by my performance as his house physician and considered I would be suitable for a career in paediatrics. Also, there was a vacancy in his department for a Senior Registrar Tutor in Paediatrics and there had been some difficulty in filling the post. I was offered the position at the grade of registrar/tutor with the offer of promotion to senior registrar grade when, and if, I obtained the Membership of the Royal College of Physicians of Edinburgh in Paediatrics (MRCPE).
This offer was, to put it mildly, a bombshell! Here I was, a mere surgical Senior House Officer, hardly yet started on a surgical career, satisfactory progress in which was by no means certain, being offered a registrar job in the University Department of Paediatrics with the promise of promotion to senior registrar when I obtained the appropriate higher paediatric qualification i.e. the Membership of one of the Royal Colleges of Physicians.
I agreed to think this over which I did over the next 24 hours. Considered objectively I had always enjoyed working in the paediatric department, first as a student locum on a number of occasions on the ward and after qualification as the paediatric house physician for six months. Also, although keen to do surgery, I had nonetheless failed to do any work on the primary FRCS anatomy correspondence course during my 2 years National Service in Malta! The road to a surgical career would be long with years of hard work and the end uncertain.
During my time in Malta I had discussed the daunting prospect of a specialist surgical career with my commanding officer in Malta, Colonel Richards who also lived in the same St Patrick’s Officers Mess. I had a good working relationship with him and towards the end of my two years National Service in the RAMC on more than one occaision he suggested I should consider sign on as a regular soldier. If I wished to do surgery the army would pay all the necessary tuition and examination fees whilst providing me with a good salary and allowances as a captain in the Royal Army Medical Corps. I had given this tempting previous offer considerable thought but did not pursue the possibility. Although I had enjoyed my time in the army I definitely did not wish to be involved with an organisation whose basic purpose was fighting! Also if one did not happen to make it as a specialist Lieutenant Colonel and remained a major as a general medical officer, one was retired in one’s early Fifties.
So, after much thought and some doubts, when George and I met again the next day, I agreed to meet with Professor Craig. The interview went well so I moved to the Leeds University Department of Paediatrics and Child Health at the end of my 6 months with Father Ellis. When I first told Mr Ellis of my decision he was surprised but very supportive. For the rest of my time with him he moved many of the paediatric children in my direction to increase my experience! He was a very nice man and it was a very good and happy six months working in his casualty department.
To return to my first published paper.
Littlewood JM, Lewis GM The Holmes-Adie syndrome in a boy with acute juvenile rheumatism and bilateral syndactyly. Arch Dis Child. 1963 Feb;38:86-8. Free pubmed.ncbi.nlm.nih.gov/13930991/
This was the first paper I wrote with co-author, George Lewis who was a Lecturer in the department and subsequently a very good friend and colleague and teacher . George eventually became a succesful consultant paediatrician in Portsmouth with a happy family; he and lived into his Nineties
So, I was now a member of the University Paediatric and Child Health Dept with my own little office in the old house the department occupied in Blundell Street behind the Leeds General Infirmary. I was keen to start writing. Then this opportunity to write a case report came my way. Professor Craig was a very good writer with many papers and two very successful medical books to his credit, and, after he retired a biography of John Thomson, the famous Edinburgh paediatrician, whom he described as “Pioneer and Father of Scottish Paediatrics”. However, Prof. didn’t appear to encourage his juniors to publish; nevertheless George Lewis and I decided to write up this case report and we thanked Prof. for “much helpful advice”. There wasn’t the same drive to publish papers in those days.
The case report concerned a 7-year old boy. He was an inpatient in Professor Craig’s ward at Seacroft hospital with acute rheumatic fever. He also had Holmes-Adie eye syndrome with the dilated pupil on the right and syndactyly (joined 4th and 5th fingers on both sides).

Rheumatic fever is a condition we used to see in the Sixties but I have not seen in recent years although it remains a major problem in many developing countries. However, in 1963 it was a not uncommon reason for long admission to children’s wards in the UK. The condition often resulted in long term cardiac damage leading to mitral stenosis and other heart problems later in life.

Our patient had a typical attack of rheumatic fever with pyrexia, multiple very painful joint involvement and a typical erythema marginatum skin rash (figure). His resting heart rate was raised to 130 but settled during the second week; the soft systolic murmur noted on admission remained unchanged throughout. He also had absent patellar reflexes (knee jerks). Treatment consisted of complete bed rest for the first month, penicillin and salicylate (aspirin) treatment with a gradual return to normal

activity within 3 months. It appeared the Holmes-Adie pupil developed at the same time as the rheumatic fever and previously had not been noticed.
The typical Holmes-Adie pupil was first described by William John Adie an Australian born British physician and neurologist and Sir Gordon Morgan Holmes an anglo-iris neurologist independently in 1931. (Adie WJ. Tonic pupils and absent tendon reflexes: a benign syndrome sui generis: its complete and incomplete forms. Brain 1932;55:98-113)
In 1931, around the same time as Adie’s first paper on tonic pupils, Sir Gordon Holmes reported 54 cases largely gathered from the literature in 19 of which tendon reflexes were diminished or absent. This prompted Bramwell in 1936 to propose Holmes-Adie syndrome to describe the condition (Bramwell E. The Holmes-Adie syndrome; a benign clinical entity which simulates syphilis of the nervous system. Trans Med Chir Soc Edin 1936;83-92).
Damage to the parasympathetic innervation of the eye secondary to inflammation appears to be the cause – in our child presumably the tissue inflammation of the acute rheumatism. Absent patellar reflexes are also part of the syndrome.
Addendum: The story does not end here! Some years after our paper was published, I received a letter suggesting our patient had a specific syndrome but I’m ashamed to say I cannot remember the details! However, it may be relevant the boy’s father also had syndactyly of both 4th and 5th fingers, a similar facial appearance and he also had even had rheumatic fever at the age of 7 years! So it would appear very likely the boy had inherited a dominant condition from his father. There are numerous genetic syndromes that involve syndactyly!
However, in 2020, 57 years later, I performed a search of the literature and internet and it seems almost certain that our patient had a variety of a dominant disorder – the oculo-dento-digital dysplasia (ODDD). Described as follows – “The phenotype of ODDD comprises craniofacial (short and narrow palpebral fissure, thin, narrow nose with hypoplastic alae nasi), dental (oligodontia, hypoplastic enamel), and digital abnormalities (syndactyly of finger 4/5, hypoplastic phalanges). Ocular manifestation is typical and involves microphthalmia, microcornea, glaucoma, congenital malformations of iris or vitreous, ectopic pupils or strabismus”.
There are now (in 2021) 191 publications involving ODDD in the literature including evidence that ithe condition is caused by mutations in the GJA1 gene in chromosome 6q22 and inherited in an autosomal dominant manner in the majority of the patients. The first description of the syndrome was in 1963 – the same year as our publication – by Gorlin RJ, Miskin LH, St Geme JW. Oculodentaldigital dysplasia. J Pediatr 1963; 63:69-75. Their summary is as follows- “A new syndrome, oculodentodigital dysplasia, is presented. Six case histories, 5 found in the literature and 1 of our own, have been analysed and found to demonstrate similar changes. This new symptom complex is characterized by ocular anomalies which include hypotelorism, microphthalmia, and iridic changes; digital disfigurations including syndactyly and camptodactyly of the fourth and fifth fingers, and hypoplasia or aplasia of the middle phalanges and toes; and severe hypoplasia of the enamel of all the teeth. No chromosomal anomaly was demonstrable and no genetic pattern of transmission was apparent”.

Robert James Gorlin, DDS PhD (1923-2006) was described as a world-renowned oral pathologist, human geneticist and academic at the University of Minnesota School of Dentistry. In 1956 he joined the faculty at the University of Minnesota School of Dentistry, Minneapolis, as an associate professor and chair of the divisions of oral histology and oral pathology. At the time of his death, he was the UM Regents’ Professor Emeritus of Oral Pathology. He published over 600 articles in a variety of topics, and held joint appointments with the University of Minnesota’s departments of pediatric medicine, laboratory medicine and pathology, obstetrics and gynecology, otolaryngology and dermatology.
There are numerous images on the ODDD website and I now have little doubt that our boy had the ODDD syndrome. It is relevant that our paper was published in 1963 – the same year ODDD was first described as a distinct syndrome by Robert Gorlin. I suspect it could have been Gorlin who wrote to me suggesting our boy had the syndrome he had just described. Sadly we will never know.
Littlewood JM. Polycythaemia and Anaemia in Newborn Monozygotic Twin Girls. Br Med J. 1963 Mar 30;1 (5334):857-9. Free pubmed.ncbi.nlm.nih.gov/20789723/


These twins were born at the Leeds Maternity Hospital and full details are in the free version of the paper. Their appearance was quite remarkable – the smaller first twin being very cyanosed with a Haemoglobin 25.6G/100ml (175%): the larger second twin was very pale with an Hb of only 7.8G/100 (52%). The placenta conformed to previous descriptions of the syndrome with one very engorged side the other being very pale. We performed an exchange transfusion for the first plethoric twin to correct the polycythaemia and gave a standard blood transfusion to the second anaemic twin. Their subsequent progress was normal.
The parabiotic syndrome is the most common serious complication of monochorionic twin pregnancies, with perinatal mortality rates of up to 90% if untreated. Article written by Kurt Benirschke, MD from the UCSD University Medical Center and founding member of The Twin to Twin Transfusion Syndrome Foundation’s Medical Advisory Board described the first delineation of twin to twin transfusion syndrome was by a German obstetrician, Friedrich Schatz. In 1875 he described the placental “third circulation” and more fully explored this concept in 1886. Schatz injected the fetal placental blood vessels of twins and showed clearly that there are inter-twin blood vessel anastomoses, most commonly artery-to-artery communications. These occurred only in “identical” twins, and only in those (2/3) who possessed a so-called monochorionic twin placenta. But, when he further studied the vascular anastomoses, he saw that there occurred also artery-to-vein communications. Because these traveled from one twin to the other, the possibility of “transfusion” from one twin to the other was assured. These transfusions took place through a “villous district” of the placenta and, because they could not be seen directly from a surface inspection of the blood vessels in the placenta, he called this the “third circulation”. Then, he made a remarkable discovery. He saw a set of twins with the classical twin to twin transfusion syndrome and described this in a very long meticulous paper.
More recently surgical correction using laser photocoagulation of communicating placental vessels was developed in the 1980s and refined in the 1990s. Survival of one or more foetuses following laser surgery is currently more than 90%, however, the neurodevelopmental outcomes for survivors remains unclear in from 4 to 31%. I have no information on the long term progress of our twins but from followup notes it appears to have been normal.
Littlewood JM. Kohler HG. Urinary tract infection by Trichomonas vaginalis in a newborn baby. Archives of Disease in Childhood. 41(220):693-5, 1966 Dec. pubmed.ncbi.nlm.nih.gov/5927928/ Free
This is a report I wrote with Dr Hans Gerhart Kohler (1915-2004). He was the perinatal pathologist at the Leeds Maternity Hospital (1963-80) when I was lecturer in paediatrics working for Prof Craig at the hospital. This infection was identified during a screening survey of newborn infants urine I was carrying out in the Leeds Maternity Hospital; the results of the main survey are discussed later in this Paper Trail
Hans Kohler (1915-2004) was a lovely man and a meticulous worker; he and his laboratory staff were very supportive of the clinical staff. He had an interesting personal and family history mentioned in his BMJ obituary in 2004 “His early life reflected the turmoil in central Europe caused by two world wars. A free thinker, he became an atheist aged 12 and a Young Communist at 15. He was politically active while a medical student and when fascism darkened Czechoslovakia, he decided to leave. Using false papers he was on the last Kinder transport for Holland. Once in Britain he enlisted in the Czech army-in-exile, becoming a Royal Army Medical Corps captain. His parents survived Auschwitz, but his only brother died on the forced march from Auschwitz to Dachau. Hans married twice—to Anna and later, as a widower, to Hanna. He leaves three children”
I will always have pleasant memories of Hans. I also remember one evening he asked Ann and myself to his flat in North Leeds for a meal. After drinks he left for a short time and returned with a box of Colonel Sanders Kentucky Fried Chicken ! It has remained a great favourite of mine ever since!

Trichomonas vaginalis is an anaerobic flagellated protozoan that can cause genital infection. This infant presumably acquired the infection during birth during his passage through the birth canal. Diagnosing infection from voided urine in infants was always open to question as the organisms may have entered the urine during voiding. This case report seems convincing that this is a genuine urinary infection rather than from perineal contamination; this case was reported before I used suprapubic bladder aspirations to confirm urinary infections in young infants. In this infant the positive urine findings had persisted until the 64th day when oral treatment with metronidazole 50 mg thrice daily for 7 days was started and proved rapidly effective in eradicating both the parasite and the pus cells from the urine. The immediate response to treatment of the Trichomonas vaginalis in the urine after so many positive cultures and its association with significant number of white blood cells all support a genuine infection. The infant, the urine and intravenous pyelography of the urinary tract were all normal at the age of 4 months.
Littlewood JM. Candida infection of the urinary tract. Case report, with a review of the literature and a study of frequency of yeast isolations from the urine of children with bacterial urinary infections. British Journal of Urology. 40(3):293-305, 1968 Jun. pubmed.ncbi.nlm.nih.gov/4872410/
This is a case report and an extensive review of the previous literature relating to Candida urinary infections.
To digress for a moment. In 1968 a “review of the literature” was a laborious task. Today, in 2025, one would go straight to the internet and search the PubMed database where all the previous publications relating to the subject would be listed, most with summaries and some with access to full texts. However, in 1968 such a search involved walking to the medical school library, consulting the Index Medicus, writing details from the previous references to the subject of interest on index cards (there were no photocopiers then). One would then get the appropriate bound journal from the shelf (if the library subscribed to the journal). To obtain a full text of the article one would write to the author politely requesting a “reprint”. Most authors received a number of free copies of their articles from the publisher and would order and purchase additional copies to respond to such requests. It is true the literature was less extensive in 1968 when there were less than 20 publications on this subject than in 2020 when there were 1090 recorded in PubMed! However, I managed to find 50 references relating to candida in the urine from various sources at the time of this paper.

In the present infant the diagnosis was established beyond doubt by finding more than 100,000 viable candida units per ml in two catheter urine specimens. There were predisposing factors including significant anatomical abnormalities of the urinary tract, use of many antibiotics including a period of neutropenia following chloramphenicol therapy. Alkalisation of the urine resulted in a marked reduction in the number of yeasts which returned when the alkali was discontinued. The yeast eventually cleared spontaneously.
I received considerable help from Dr Charles J T La Touche, who was the consultant mycologist in Leeds at the time, who wrote the Methods section of my paper. He was most helpful, not only with the laboratory investigations but also with the treatment of this boy who had an anatomically abnormal urinary tract associated with spina bifida.
Charles La Touche (1904-1981) had an interesting history. He was born in China, returned to Europe by the Trans-Siberian railway, went to school in France and England, and graduated in science from Dublin in 1924. He then worked as mycologist at St Mary’s Hospital, London, under John Freeman who was then interested in allergy induced by house dust and fungal spores . Apparently, it was a spore from one of La Touche’s cultures which contaminated a bacterial culture in Alexander Fleming’s laboratory on the floor above that led to the discovery of penicillin. Then, for a period La Touche was mycologist to the Mushroom Growers’ Association after which, wishing to take up medical mycology, at the age of 42 years La Touche qualified himself in medicine in Dublin in 1946. The next year he was appointed senior lecturer in medical mycology at the University of Leeds under John T. Ingram a distinguished local dermatologist. La Touche published on a variety of mycological topics when at Leeds. He was a President of the British Society for Mycopathology for 1960.
At the time of our paper I had not realised that Dr Charles la Touche had been engaged in research at St Mary’s Hospital, London, in the Thirties. In 1978 he was an honoured guest at a meeting at St Mary’s which marked the fiftieth year of the “Antibiotic Era”. At the end of his original 1929 description of penicillin (in the British Journal of Experimental Pathology 1929; 10:226-236), Alexander Fleming writes – “In conclusion my thanks are due to my colleagues Mr Ridley and Mr Craddock for their help in carrying out some of the experiments described in this paper, and to our mycologist, Mr la Touche, for his suggestions as to the identity of the penicillium”.
I was unaware of any of this during my collaboration with Dr La Touche – he was just a very quiet, unassuming and helpful man from the mycology department! (Some of these details are from Geoffrey C Ainsworth’s Brief Biographies of British Mycologists).
Littlewood JM. Asymptomatic bacteriuria. British Medical Journal. 3(667):416, 1969 Aug 16. Letter pubmed.ncbi.nlm.nih.gov/5797794/
This was a letter I wrote to the BMJ commenting on a recent study by Dr Roy Meadow. I did not know Roy at that time but when he moved to Leeds, first as Senior lecturer with Professor Dick Smithells and then as Professor at St James’s, we wrote a number of papers together and became good friends and colleagues. We were both very interested in urinary tract infections and the potential damage to the kidneys. I later moved on to other subjects. Roy eventually took over my urinary clinic as that was one of his special interests.

The present paper of Roy’s described screening school childrens’ urine for the presence of pus cells (Meadow SR et al, Prevalence of symptomless urinary tract disease in Birmingham schoolchildren. 1 Pyuria and bacteriuria. Br Med J 1969 Jul 12;3:81-4. PMID 5790270). Using Labstix commercial test strips and microscopy, a urine specimen was considered abnormal if it gave an albumin reading of one-plus or more, a positive occult blood or glucose test, or contained erythrocytes or more than 10 leucocytes (pus cells) per cu.mm – there was no mention of bacteria. This was surprising, for as the urine was microscoped, even if not stained, bacteria would have been visible as a direct indication of bacteriuria. Another study by Dennis Savage in Bristol found only 60% of proven bacteriuria specimens contained significant numbers of pus cells (pyuria) – so pyuria is an insensitive method of identifying bacteriuria – this was the point of my letter.

I subsequently published a study showing the value of direct urine microscopy for identifying bacteria which I had learned originally from Dr Hughes–Davies, the excellent Senior Registrar I worked with when I was an SHO at Great Ormond Street in 1963. I further commend the use of direct microscopy to identify bacteriuria on which I later published (Littlewood JM et al. Arch Dis Child 1977 Nov; 52(11):894-6. Free).
I even suggested that school medical officers should screen children’s urine by direct microscopy at school medical examinations (it never happened!!). Children so identified could form the basis of a study on the natural history of asymptomatic bacteriuria which was needed; it could not be deduced from children attending special clinics for pyelonephritis nor from the incidence of renal scaring at different ages. At that time there was much interest in the long term damaging effects on the kidneys of urinary infections in childhood causing ureteric reflux.
Dickinson JP. Holton JB. Lewis GM. Littlewood JM. Steel AE. Maple syrup urine disease. Four years’ experience with dietary treatment of a case. Acta Paediatrica Scandinavica. 58(4):341-51, 1969 Jul. pubmed.ncbi.nlm.nih.gov/5824823/
John Dickinson was a chemical pathologist at the Leeds General Infirmary; John Holton also a biochemist; Alan Steel was the biochemist at Seacroft Hospital at the time. There was also major input from the nursing staff and paediatric dietitians.
An, as yet undiagnosed, drowsy 3 week old full term infant was transferred from the Leeds Maternity Hospital Special Care Baby Unit to the paediatric ward at Seacroft Hospital for further care and investigation. After a normal pregnancy weighing 3150 g the infant had appeared normal up to the age of 5 days after which she became increasingly more lethargic to the extent she was unable to suck. She had four convulsion on the at the end of the first week. Various investigations including subdural taps and a ventricular aspiration by a neurosurgeon proved negative. Her comatose condition continued and she was transferred to Seacroft hospital for further care. It was a most unusual clinical picture.
Soon after the infants’s arrival our ward at Seacroft our excellent Ward Sister, Jean Wilson, commented on the unusual yeasty smell particularly from the infant’s nappy. So a specimen of urine was sent to the laboratory for analysis. Alan Steel, our Seacroft Biochemist, examined the urine for amino acids and found an excess of the amino acids leucine, isoleucine, valine and diagnostic of Maple Syrup Urine disease.

The condition was of the same nature as phenylketonuria but more complex involving inability to handle three amino acids leucine, isoleucine and valine. At the time, in 1968. we had never heard of the condition which had been described by an American neurologist John Menkes in Pediatrics in 1959 https://pubmed.ncbi.nlm.nih.gov/13633350/
The complex dietary treatment and biochemical monitoring to control the levels of the three amino acids was started for our patient from the age of six weeks with a synthetic diet containing carefully restricted quantities of the three branched chain amino acids leucine, isoleucine and valine. There was a marked immediate improvement. At twelve weeks gross vitamin deficiency developed and was corrected. By the age of four-and-a-half years she was in reasonable general health but quite severely retarded, both mentally and physically. After the publication of the report the patient contracted a respiratory infection: there followed a rapid clinical and biochemical deterioration. Despite intensive therapy she died of bronchopneumonia.
Fortunately from 2014 all newborns in the UK were screened for MSUD by identifying high levels of leucine and isoleucine in the blood spot and dietary treatment can start before brain damages occurs in much the same way as occurs with phenylketonuria. Apparently a liver transplant is sometimes an option to treat MSUD. If a person with MSUD receives a donated liver, they’ll no longer be at risk of a metabolic crisis and can have a normal diet. However, liver transplantation is not considered a cure for MSUD. The patient will still carry two copies of the mutated BKAD gene in each of their own cells, which will consequently still be unable to produce the missing enzyme.
Addendum: Some years after this infant was treated, during the Seventies, an experienced consultant paediatrician from a nearby Yorkshire city brought a baby, with a yet undiagnosed condition, to our weekly paediatric meeting for consultants at Seacroft for suggestions as to the diagnosis. As soon as I entered the cubicle where the baby was being examined I immediately recognised the odour of maple syrup having smelt it previously, and sadly too late, with our unfortunate infant. With confidence I told him the diagnosis was maple syrup urine disease which at first he couldn’t believe. I wonder how it was we could have missed that very characteristic smell for a number of weeks with our previous unfortunate infant until June Wilson our excellent ward sister noticed it.
Littlewood JM. Kite P. Kite BA. Incidence of neonatal urinary tract infection. [ Journal Article] Archives of Disease in Childhood. 44(237):617-20, 1969 Oct. pubmed.ncbi.nlm.nih.gov/4981204/
[The first description of transient bacteriuria in newborns] This was one of the main papers from my MD thesis “Urinary infection in the newborn with special reference to variations in symptomatology and ultimate prognosis”. MD Thesis Leeds University 1968.
Essentially it was a screening survey of 600 infants at the Leeds Maternity Hospital carried out over 125 days between April and August. Eight infants (7 boys) were found to have urinary infections – an overall incidence of 1.4% (boys 2.3%, girls o.3%). All had signs so mild that in all probability they would have been overlooked had the survey not been in progress. The frequent occurrence of transient mild urinary infection, particularly in male infants was stressed. This data was included in my MD thesis.

During the course of the study I went to the Maternity Hospital every morning before work. In the small laboratory side room on the Special Care Baby Unit (SCU) over the entrance, I microscoped, performed cell counts and set up cultures on all the urine specimens the really helpful and interested midwives had collected for me the previous day. I thanked particularly the sisters and nurses at the Leeds Maternity Hospital for their interest, and their skill at collecting mid-stream urine specimens from so many newborns. In particular, Sister M Pattullo the formidable senior sister of the SCU, was very supportive and great source of information and wisdom. (This was the only photo of her I could find!)
It was a pleasure to work with Mr Peter Kite, then Senior Laboratory

Scientific Officer at Leeds Maternity Hospital ,who suggested the method of bacterial counting and taught me the technique. Peter’s wife Beverley Kite also assisted me in the laboratory with examination of some of the the specimens.
Peter Kite subsequently had a varied and distinguished career and was involved in a further 40 publications from 1969-2009 working in the Leeds Teaching Hospitals and as an independent research scientist.
Dr (later Professor) William Brumfitt (1929-2020), at the time an acknowledged expert on urinary infections, gave me much helpful advice in planning the survey.

Our insurance agent in Leeds was Professor Brumfitt’s elder brother and he knew my father many years ago when he was Manager of the Century and Friends Provident Building Society in Leeds. During conversation with Mr Brumfitt about our family insurance at the time in the Sixties I mentioned I was planning this survey. He said “My young brother Billy in London is an expert on urinary infection – I’ll ask him if he can advise you”. And so he did and “Young Billy’ was most helpful in the planning of the study and identifying the serotypes of the organisms we isolated.
Prof. William Brumfitt had a varied and very distinguished career eventually being appointed to the chair of medical microbiology at the Royal Free Hospital, London.
I believe asymptomatic bacteraemia (transient presence of bacteria in the blood stream) may well be a relatively common occurrence in the first few days of life during the initial bacterial colonisation of the infant as suggested by Albers W H et al. (J Pediatr 1966;69:193. PMID:5946646) and transient urinary infection may be one manifestation of this. The relation to later renal disease is unknown, although none of these neonatal infections were associated with significant anatomical abnormalities.
The nursing staff at the Leeds Maternity Hospital took a great interest in the survey and became expert at collecting midstream urines from neonates.

They shared our excitement as the infants with urinary infection were identified.
It was during this survey I first performed suprapubic bladder aspirations – I will never forget the first occasion that obviously infected turbid urine entered the syringe; then, in the side room of the Special Care Baby Unit, placing a drop on a microscope slide under a cover slip and observing millions of motile bacteria
Littlewood JM. White cells and bacteria in voided urine of healthy newborns. Archives of Disease in Childhood. 46(246):167-72, 1971 Apr Free pubmed.ncbi.nlm.nih.gov/5576025/
During my screening survey for urinary infection in the Leeds Maternity Hospital, 600 infants had one or more urines examined by me on the sixth or seventh day of life and 592 were subsequently shown to be uninfected. Every infant who was in the Leeds Maternity Hospital at the age of 6 days and who was not receiving antibiotic therapy was included.
The survey lasted 125 days between April and August 1967. Urine specimens were collected by the midwives either in the lying-in wards or in the special care baby unit. This was for my MD thesis so I personally examined all the urines either before or after routine work, weekends included, between April and August 1967 – heavy going! The paper contains details of white cell counts and bacterial counts from bag urines and clean catch specimens.
Littlewood JM. 66 infants with urinary tract infection in first month of life. Arch Dis Child 47(252):218-26, 1972 Apr. pubmed.ncbi.nlm.nih.gov/5023470/
This was a retrospective analysis of sixty-six newborn infants with urinary tract infection in the excellent neonatal records of the Leeds Maternity Hospital. The wide variation in clinical manifestations is stressed and suggested as an explanation for the variety of clinical descriptions, incidence and prognosis noted by previous authors.
The condition commonly presents on the sixth or seventh day, there is no seasonal incidence, boys are affected more frequently than girls. There was a correlation with maternal infection, perinatal anoxia, and birth weight either below or above the normal range. Unsatisfactory weight progress, lethargy, and anorexia were the most frequent clinical signs. The overall mortality was 11% and further infection occurred in 37% of girls and in none of the boys.
Littlewood JM. Letter: The prevalence of bacteriuria in full-term and premature newborn infants. [ Journal Article] Journal of Pediatrics. 83(5):888-9, 1973 Nov. pubmed.ncbi.nlm.nih.gov/4742588/
Addy D. Littlewood J. Ventricular tachycardia associated with hyperkalemia. Occurrence in an infant aged 13 days with adrenogenital syndrome. American Journal of Diseases of Children. 117(6):706-9, 1969 Jun. pubmed.ncbi.nlm.nih.gov/5771512/

This was the first reported example of ventricular tachycardia occurring in a newborn infant. An outwardly normal male infant was reluctant to feed and gain weight from the 5th day of life. When admitted aged 13 days he was cyanosed and mildly dehydrated. The cardiac rate was 104 per minute and rhythm was abnormal with runs of bigeminal rhythm (figure). The external genitalia were normal.The serum electrolytes were abnormal – serum sodium 120 (normal 134-160), potassium 9.4 (n 5-7.7) and chloride 90 (n 93-112) mEq/litre. A provisional diagnosis of salt loosing adrenogenital syndrome was made.
Adrenogenital syndrome, also known as congenital adrenal hyperplasia, is a group of autosomal recessive disorders which result from disorders of steroid hormone production in the adrenal glands, leading to a deficiency of cortisol. The pituitary gland reacts by increased secretion of corticotropin, which in turn causes the adrenal glands to overproduce certain intermediary hormones which have testosterone-like masculinising effects.
In female infants there is masculinisation of the external genitalia with enlargement of the clitoris which may initially cause difficulty in deciding the sex of the infant but it does allow early recognition; these genital changes are not obvious in the newborn male infants as was the case in our present infant.
Our infant was treated with an intravenous infusion of 0.45% saline and hydrocortisone. After a variety of ECG changes (figure) the heart rate normalised in 12 hours. The diagnosis of adrenogenital syndrome was confirmed by raised urinary 17-ketosteroids, 17-hydroxtcorticosteroids and pregnanetriol. His progress was eventually satisfactory on cortisone acetate 7.5 mg thrice daily, fludrocortisone acetate 0.025 mg twice daily and sodium chloride 1.0gm daily

Douglas Addy, was tutor in Prof. Craig’s paediatric department at the time. Our families remained friends for many years. Doug, after working in London at the Hammersmith and then Baltimore at Johns Hopkins, was appointed consultant paediatrician at Dudley Road Hospital in Birmingham. We are still in contact with Doug – in fact, Ann had contact with him regarding a PowerPoint presentation for a history society lecture as recently as 2020. Jennifer died some years ago.
Littlewood JM. Spina bifida. Nursing Times. 66(1):5-8, 1970 Jan 1. pubmed.ncbi.nlm.nih.gov/4903383/
This was a substantial article covering the management of infants with spina bifida iat the time which had undergone considerable changes in the preceding years.


During the Sixties, when I was in Professor Craig’s department, I was given the responsibility of seeing all infants born with spina bifida as soon as possible after birth. There was evidence from Dr John Lorber in Sheffield that early surgical treatment with closure lessened the physical handicap and reduced the early infection of the lesion.
So I examined many infants with spina bifida soon after birth. Subsequently many came to a combined clinic I organised for children with urinary infections and spina bifida. Nurses, doctors and other workers in various aspects of management would see these children and their parents regularly – a neurosurgeon (Mr. Myles Gibson), an orthopaedic surgeon (Mr. Pasco Clark) and urologist (Mr. Bob Williams) all attended my clinic regularly.

Supervision of the back lesion, the hydrocephalus and the ever present danger of urinary infections continues throughout the first year. Many of the children developed hydrocephalus and needed a Spitz-Holter or Pudenz vale to relieve the intracranial pressure.
In the second year orthopaedic treatment aimed to result in a pair of straight limbs with reasonably stable joints suitable for fitting callipers and the child should be attempting to stand and walk.
The subsequent course was very complex and such children with all their associated problems of the spinal lesion, the hydrocephalus, the neurological involvement of the lower limbs – both motor and sensory – and the urinary tract abnormalities represented an increasing proportion of the physically handicapped school population and at the time.
At that time in the UK 1-2/1000 infants were born with spina bifida and 70-80% were likely to survive with modern surgical treatment. Unfortunately, most survivors had continual medical, educational and social problems.


Previously, before the Sheffield early treatment approach of Dr John Lorber(1915-1996) and Mr Bob Zachary (1913-1999) only 10% of those born alive survived to school age. Undoubtedly, the recent increase in survival at the time of this paper was due to the introduction of closure of the back lesion and control of the hydrocephalus with a valve if required.
John Lorber eventually changed his opinion about active treatment in view of the very poor long term outlook – this was not popular with the pro-life groups.
Addendum. Some facts about the spina bifida situation in 2024
Professor Dick Smithells (1924-2002), Prof. Craig’s successor in Leeds, carried out research on nutrition in pregnancy as one of his main projects . He started Leeds Pregnancy Nutrition Study in 1969 and published a report in 1976. (Smithells RW, Sheppard S, Schorah CJ. Arch Dis Child 1976; 51:944. Vitamin deficiencies and neural tube defects https://pubmed.ncbi.nlm.nih.gov/1015847/)

In 6 mothers who gave birth to infants with neural tube defects, serum folate, red cell folate, white blood cell vitamin C, and riboflavin values were lower than in controls. In spite of small numbers the differences were significant for red cell folate (P<0.001) and white blood cell vitamin C (P<0 .05). The authors suggested these findings are compatible with the hypothesis that nutritional deficiencies are significant in the causation of congenital defects of the neural tube in man.
The authors subsequently conducted a study of pre-conceptional vitamin supplementation of mothers who have already had one or more infants with CNS defects. (Smithells et al, Lancet 1980 Feb 16;8164:339-40)https://pubmed.ncbi.nlm.nih.gov/6101792/) Women who had previously given birth to one or more infants with a neural-tube defect (NTD) were recruited into a trial of preconceptional multivitamin supplementation. 1 of 178 infants/foetuses of fully supplemented mothers (0.6%) had an NTD, compared with 13 of 260 infants/foetuses of unsupplemented mothers (5.0%).
I recall hearing Dick Smithells present this data at a lunch time meeting at our St James’s weekly paediatric meeting. It was quite dramatic, a positive result after 10 year’s work; I remember congratulating him warmly on what was a quite dramatic and very important result.
There were continuing discussions and publications about this paper and Smithells expanded the finding in his last 1981 paper discussed in 2011 publication (Smithells et al. Apparent prevention of neural tube defected by periconceptional vitamin supplementation.1981 Int J Epidemiol 2011;40:1146-54)
An earlier preliminary paper is expanded. Women who had given birth to one or more infants with a neural tube defect were recruited into a trial of periconceptional vitamin supplementation. Two hundred mothers attending five centres were fully supplemented (FS), 50 were partially supplemented (PS), and 300 were unsupplemented (US). Neural tube defect recurrences in the study pregnancies were 1(0.5%), in FS, none in PS, and 13 (4%) in US mothers. The difference in outcome between FS and US mothers is significant. The most likely explanation is that supplementation has prevented some neural tube defects, but further studies are needed.
Smithells work led to the larger “MRC Vitamin Study” in 1983 which ended early in 1991 due to positive conclusive results. There was a 72% protective effect of using folic acid daily in an intention-to-treat analysis and an 83% protective effect in an on-treatment analysis. There was no evidence that the other seven vitamins in the formulation used by Smithells and his colleagues had any effect. Critics had claimed that the trial was unethical even though there remained uncertainty as to whether any vitamins, let alone folic acid, could prevent neural tube defects. However, Sir James Gowans, the then Secretary of the Medical Research Council, recognised the need for the trial and stewarded it through a barrage of hostile press and political commentary.(MRC Vitamin Study Research Group. Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. Lancet 1991;338:131-7).
In my opinion it is absolutely deplorable that mandatory fortification of flour with folic acid was still (in 2024) not routine in the UK even though significant reductions in incidence have occurred in many of the 81 countries who were sensible enough to introduce mandatory folic acid flour fortification.
As far back as 2011 Professor Nick Wald observed –
“Smithells, who died in 2002, was delighted that his lifelong work led to the opportunity to prevent most cases of serious birth defects, but he would have been saddened that his own country had done so little in delivering the benefits of British research to its own population”.
The subject has been recently reviewed in 2018 by Wald et al (Public health failure in the prevention of neural tube defects: time to abandon the tolerable upper intake level of folate. Public Health Rev. 2018 Jan 31;39:2.PMID:29450103) who showed that “the scientific basis for setting any upper limit folate intake, let alone one at 1 mg/day, is flawed. An upper intake level is therefore unnecessary and should be removed, thus allaying unjustified concerns about folic acid fortification. As a result, the full global opportunity to prevent two serious fatal or disabling disorders can and should be realised”
In 2018 Nick Wald concluded “failure to fortify flour with folic acid is more than a missed opportunity; it is a tragedy. Since 1991, it has been estimated that there have been over five million preventable NTD pregnancies in the world.”
Most recently Nicholas Wald, Joan K Morris and Colin Blakemore (a powerful and respected trio) published their answers to the Government’s nine questions when the subject of flour fortification was put out for public consultation (Wald et al. Urgent need for folic acid fortification of flour and grains:response to the 2019 UK Government’s public consultation. Arch Dis Child January 2020; 105:6-9. PMID: 31843795)
This review sets out and answers in detail the nine main questions. Their aim is to present the rationale for mandatory fortification, what products should be fortified and the mean daily folic acid intake increase fortification should achieve across the population.
In late 2024 the UK government were still consulting on the subject! See Below

Professor Nicholas Wald is a research physician and epidemiologist who specialises in preventive medicine. In the 1970s, he introduced the pioneering concept of screening pregnant women for congenital disorders, or birth defects — initially spina bifida and later Down’s syndrome. Surprisingly he later opposed the introduction of neonatal CF screening but supported antenatal screening. Ironically, neonatal screening was approved by the government in 2001 became nation-wide by 2007 and national antenatal CF screening has not been introduced in the UK by 2021!
I apologise for going into such detail and with such vigour on this subject of neural tube defects but extensive personal experience as a paediatrician looking after these unfortunate children with spina bifida from their first days, breaking the news to their parents and following them and their families in my clinic makes one angry at the unnecessary suffering that has resulted from failure to introduce folic acid supplementation in the UK.
As Wald observed in 2018 “While the thalidomide tragedy prompted immediate worldwide public health intervention, many countries still ignore the preventable toll of disability, stillbirth, infant death, and terminations of pregnancy caused by neural tube defects”.
At last !!! From:Department of Health and Social Care, Department for Environment, Food & Rural Affairs, New legislation being introduced today will require millers and flour producers to fortify non-wholemeal wheat flour with folic acid from the end of 2026.
- Folic acid to be added to non-wholemeal flour to protect newborn babies from serious brain and spine problems
- Move will prevent around 200 cases of neural tube defects every year and improve health of pregnant women
- Measures to come into force at the end of 2026 to help businesses prepare.
Littlewood JM. Hunter I. Payne RB. Miles DW. Placental transfer of an IgG paraprotein associated with prolonged immunosuppression. British Medical Journal. 4(727):94-5, 1970 Oct 10.Free pubmed.ncbi.nlm.nih.gov/5471777/
Please see next abstract for followup
During my screening survey of newly born infants for urinary tract infection 8 out of 600 infants investigated were found to have a significant bacteriuria (Littlewood MD thesis). Plasma protein electrophoresis was carried out as part of the survey on these 8 infected infants, and in one of them, a boy aged 6 days, a deficiency of normal IgG was associated with the presence of an IgG type K paraprotein. The plasma of the mother was therefore investigated and a previously unsuspected asymptomatic paraproteinaemia was discovered.
 A paraprotein is an abnormal protein secreted by a clone of plasma cells or lymphocytes. Although it can be associated with myeloma or lymphoma a paraprotein is more commonly a manifestation of a of condition called Monoclonal Gammopathy of Undetermined Significance (MGUS). Paraprotein occurs in 0.3% of the people less than 50 yrs old but increases to 10% in those over the age of 80 years. About 1% per year of those affected will develop a myeloma or low grade lymphoma (clear facts from the Norfolk and Norwich University Hospitals website).
A paraprotein is an abnormal protein secreted by a clone of plasma cells or lymphocytes. Although it can be associated with myeloma or lymphoma a paraprotein is more commonly a manifestation of a of condition called Monoclonal Gammopathy of Undetermined Significance (MGUS). Paraprotein occurs in 0.3% of the people less than 50 yrs old but increases to 10% in those over the age of 80 years. About 1% per year of those affected will develop a myeloma or low grade lymphoma (clear facts from the Norfolk and Norwich University Hospitals website).
The infant’s urinary infection responded to treatment with ampicillin and the paraprotein gradually disappeared. His subsequent progress was uneventful. His mother was in good health 2 years later. She had two courses of cyclophosphamide but the paraprotein remained unchanged.

Dr Brian Payne was a chemical pathologist at St James’s at the time and a good colleague with whom we worked on many occasions. Brian, now 89 years, old retired 25 years ago. He has practised yoga since 1967 and wrote a book called Slow Yoga in 2001 Also, with Rick Jones, he wrote a book on Clinical Investigation and Statistics in Laboratory Medicine which is still going strong. Although now a widower, Brian he has four daughters, fourteen grandchildren and two great grandchildren. It’s really amazing that I knew Brian well as a colleague for so many years but had no idea of his other activities. He is certainly a very pleasant pers
(See also the following abstract)
Littlewood JM. Payne RB. Placental transfer of IgG paraprotein with prolonged immunosuppression. [Case Reports. Letter] British Medical Journal. 1(6056):291, 1977 Jan 29. FREE pubmed.ncbi.nlm.nih.gov/837084/
This is a follow-up of a report Brian Payne, the chemical Pathologist at St James’s, and I published seven years ago (abstract above).
In 1970 we reported a transfer across the placenta of maternal IgG paraprotein which give rise to immunosuppression of the circulating concentrations of IgG IgA and IgM in the infant. The IgG and IgA concentrations were still low at two years. In this paper we report the progress of the child and mother during the subsequent seven years. During the past four years the boy, who is now nine years old, has had attacks of wheezing lasting 36 hours or so four or five times a year usually following close contact with cats or grasses. Skin testing confirmed allergies to cat dander and grass pollens. He has been otherwise well and has shown no increase susceptibility to infections.
His mother remains symptom-free and has shown no increased susceptibility to infections. The boy shows no remaining abnormality of IgG concentration. The mother’s monoclonal paraprotein of IgG type has persisted but has shown no change in concentration (total IgG 31g/l). There has been no significant change in the concentrations of IgA or IgM and there is no Bence-Jones proteinuria (Bence-Jones protein in the urine of patients suggests the possibility of myeloma).
Thus it now appears that the monoclonal IgG which was transferred across the placenta from the mother in high concentrations and caused prolonged suppression of humeral immunity was benign. The suppression has not persisted and has caused no lasting ill effects.
Davies JM. Gibson GL. Littlewood JM. Meadow SR. Prevalence of bacteriuria in infants and preschool children. [ Journal Article] Lancet. 2(7871):7-10, 1974 Jul 6. pubmed.ncbi.nlm.nih.gov/4134405/ 1035 apparently healthy infants and preschool children attending Leeds child-health clinics were screened for the presence of bacteria in their urine (bacteriuria) using micropipette colony-counts. Positive and doubtful cases were tested by suprapubic aspiration of the bladder: follow-up was complete. Only 1 boy out of 528 under five years of age had bacteriuria, a prevalence of 0·2%; but there were 4 cases among 507 girls, a prevalence of 0·8%. 3 of the 4 girls had radiological abnormalities. Half the children in the survey were in the first year of life when uncontaminated samples were often difficult to obtain, and repeat tests and bladder aspirations were frequently needed. Testing older children was much less troublesome, and it revealed 3 cases of bacteriuria out of 256 girls aged between one and five years. We concluded screening for bacteriuria of preschool girls, old enough to void urine on request, warrants further study.

This was one of the early studies of asymptomatic bacteriuria in pre-school children and was coordinated by John Davies, our paediatric senior registrar at the time.
John went on to be consultant paediatrician in Grimsby where he eventually introduced a pattern of consultant shift working in response to a shortage of junior staff. He was a very able, hard working doctor and set up pancreozymin-secretin pancreatic function tests for me at Seacroft. When he was our senior registrar at Seacroft in Leeds he arranged the weekly hospital clinical meetings for the staff. I will always remember on one occasion when there was a very poor attendance by the junior doctors John complained “These ungrateful people fail to eat from the spoon put into their mouths!”
Meadow SR. Davies JM. Gibson GL. Littlewood JM. Letter: Urinary tract infection in children of preschool age. [Journal Article] Archives of Disease in Childhood. 50(7):578, 1975 Jul. FREE pubmed.ncbi.nlm.nih.gov/1167077/
In this letter we question the high prevalence of urinary tract infection recently reported in preschool children in Glasgow (Boothman, Laidlaw and Richards, 1974 PMID:4614721). A “dipslide” technique was used and after serial dip slide and urine examinations in 1000 preschool, 9 were considered to have urinary tract infections. Their result contrasts with the lower prevalence found in a slightly larger and more credible Leeds survey published in the Lancet last year in that suprapubic confirmation was employed (Davies et al.,1974 above); also it contrasts with the findings in a recent London survey where there wAs a prevalence of 0.5% (Saxena SR, et al, Practitioner 1975;214(1208):257-260. PMID: 806907).
Dr George Gibson (1926-1998) was a distinguished medical microbiologist initially working with Sir James Howie in Glasgow. After a variety of other appointments Sir James Howie persuaded him to apply as Director of the Leeds Regional Public Health Laboratory. He was appointed and expanded the laboratory to be the biggest in the country and national reference facility for diseases such as anthrax, toxoplasmosis, tuberculosis and hepatitis with a special containment laboratory for dangerous viruses. His laboratory provided bacteriology services for Seacroft hospital and for this urine survey.
Kissach AW. Currie S. Harriman DG. Littlewood JM. Payne RB. Walker BE. Letter: Leigh’s disease and failure of automatic respiration. [ Journal Article] Lancet. 2(7881):662, 1974 Sep 14. pubmed.ncbi.nlm.nih.gov/4137785/
A case report of a child with a rare complex serious neurometabolic disorder Leigh’s disease also called subacute narcotising encephalomyopathy.
This condition usually becomes apparent in the first year of life. This condition is characterized by progressive loss of mental and movement abilities (psychomotor regression) and typically results in death within two to three years, usually due to respiratory failure. Mutations in mitochondrial DNA (mtDNA) and over 30 genes in nuclear DNA (gene SURF1 and some COX assembly factors) have been implicated in Leigh’s disease. Unfortunately I don’t have the precise details of this child. The number of authors involved reflect the rarity and seriousness of the case.

Simon Currie (1938-) qualified in 1962. He was a consultant neurologist in Leeds in 1970. He retired early to do medieval landscape surveying as botanist and a PhD on the interaction of medical practitioners, European and indigenous, particularly in British India and West Indies, 1750-1900. His wife, Jane Wynne, was a nationally known paediatrician dealing with child abuse; she died at sixty-four of Parkinson’s. Simon has been active as a poet fifteen years, with 180 published poems. I remember Simon as a very witty individual with a dry sense of humour. Also I will not forget when I was in my first weeks as a very inexperienced paediatric tutor and clearly remember Simon, then a medical student in my tutorial, asked me about Gilbert’s disease – at the time I’d never heard of it!
Dennis Gaston Frederick Harriman (1920 – ) was a distinguished neuropathologist, first Lecturer and eventually Reader in Neuropathology in the University of Leeds. He qualified in Belfast in 1943 and then served in the RAMC from 1944-1947 in India. He published on a wide variety of subjects from Congenital Cystic Disease of the Lung in 1945 (PMID:20476330) to Muscle fibrillin deficiency in Marfan’s syndrome myopathy in 2003 (PMID:12700307).
Brian Payne was a chemical pathologist at St James’s – please see 1970 & 1977 entries above for further details about Brian including a recent image he kindly provided.
Barry Walker was a consultant physician with the University of Leeds Department of Medicine.
Arrowsmith WA. Payne RB. Littlewood JM. Comparison of treatments for congenital non-obstructive non-haemolytic hyperbilirubinaemia. [Journal Article] Archives of Disease in Childhood. 50(3):197-201, 1975 Mar. Free version available.pubmed.ncbi.nlm.nih.gov/1147651/
Congenital non-obstructive non-haemolytic hyperbilirubinaemia (Crigler-Najjar disease) is characterized b the presence of high levels of unconjugated bilirubin in the blood resulting from a congenital deficiency of glucuronyl transferase activity. Mutations in the UGT1A1 gene cause Crigler-Najjar syndrome. This gene provides instructions for making the bilirubin uridine diphosphate glucuronosyl transferase (bilirubin-UGT) enzyme, which is found primarily in liver cells and is necessary for the removal of bilirubin from the body.
Our patient Susan was born at 36 weeks gestation 1971 after an uncomplicated pregnancy and labour. Her parents are Pakistani and unrelated. parents and 3 older daughters are well. She appeared normal at birth and weighed 2183 g. Jaundice was first noticed at 16 hours and progressed despite phototherapy and an exchange transfusion was performed on day 5. Thereafter she required long term phototherapy and was transferred from St Mary’s Maternity Hospital Bramley to Seacroft which essentially became her home. She was extensively investigated to exclude the causes for her prolonged jaundice.
At the time of this report she was 2 years old. She remained jaundiced with bilirubin ranging from 10-28 mg/100ml. Despite prolonged hospitalisation her mental and physical development have been well within normal limits. During this period various other treatment were tried – aspartic acid, a high fat diet, phenobarbitone, uridine di-phoshoglucose, cholestyramine and agar – as illustrated in the figure. We found cholestyramine to be the most successful and most easily applied supplement to phototherapy.
During this period various other treatment were tried – aspartic acid, a high fat diet, phenobarbitone, uridine di-phoshoglucose, cholestyramine and agar – as illustrated in the figure. We found cholestyramine to be the most successful and most easily applied supplement to phototherapy.
This was a very sad case of an Asian girl born at St Mary’s Maternity Hospital in Leeds. This report is of the first 2 years which she spent mostly in hospital. Ultimately she received much of her phototherapy at home with the cooperation of the Medical Physics Department. She died in teenage. Had she survived she would have received a liver transplant – pioneered by Thomas Starzl during the Sixties and Seventies but rapidly developed in the early Eighties when cyclosporin became available to prevent rejection.

Professor Grant Lathe (1913-2007) of the Chemical Pathology, University of Leeds, is described as “a pioneer in clinical biochemistry with a strong social conscience” With CRJ Ruthven he invented the technique of gel filtration now used world wide. Colin Ramsden, bacteriology and K R Johnson at St James’s examined agar for percentage inhibition of bacterial degradation of bilirubin; Dr John Holton of Bristol examined the mother’s serum for conjugation inhibitors. The nurses at Seacroft cared for Susan enthusiastically throughout and essentially provided a home for her.
Dr Bill Arrowsmith was my Senior Registrar at the time. A very quiet kind doctor. When he started we discussed a project for him. He was keen to study use of surfactant in respiratory distressed infants. “That’ll never come to anything” I said – why not study Susie our girl with Crigler-Najjar syndrome – so he did. He always reminds me, with a wry smile, of how very important surfactants became! He became a consultant in Doncaster and for many years I did a combined Cystic Fibrosis clinic with him there every few months.
We published a follow-up report on Susan in 1983 described below –
Yohannan MD, Terry HJ, Littlewood JM. Long term phototherapy in Crigler-Najjar syndrome. Arch Dis Child. 1983 Jun; 58(6): 460–462. pubmed.ncbi.nlm.nih.gov/1147651/

Now a 10 year old girl with type 1 Crigler-Najjar syndrome has been treated with daily phototherapy from birth. Her general physical and neurological development are normal. She had the general appearance of a normal Asian girl apart from moderated jaundice.
She had received daily phototherapy since the second day of her life usually for 12 hours but sometimes more. She was in hospital for the first 4 years and then at home. The domiciliary nurse collected blood samples for bilirubin twice weekly.If the level was over 350umol/l the phototherapy was increased to 16 hours.
A very difficult and abnormal lifestyle for a child but there was no alternative at the time. Understandably non-compliance was suspected on a number of occasions when the bilirubin rose and the level fell rapidly when she was admitted to hospital. The necessity for nakedness upset the Pakistani family but this was solved by an under bed light source.
Dr David Yohannan is now the Division Chief Newborn Medicine/Neonatologist at Dayton Chidren’s Hospital Ohio.
Eastham DG. Littlewood JM. Burton D. Monoparesis following CPAP. Letter: Archives of Disease in Childhood. 50(8):668-9, 1975 Aug. FREE pubmed.ncbi.nlm.nih.gov/1106335/
 A report an example of monoparesis as a complication of continuous positive airways pressure with a head box (figure). A male infant birth weight 2190 G at 35 weeks gestation developed respiratory distress syndrome at 34 hours. He was placed in a Vickers head box with maintained pressure of 10 cm. A “head box” is used for babies who can breathe on their own but still need extra oxygen. A hood is a plastic dome or box with warm, moist oxygen inside. He remained in the box gradually improving until the six days when his progress was complicated with staphylococcal septicaemia. With antibiotics he slowly improved and as he was becoming more vigorous by the 12th day abnormality of the left arm was noticed there was a complete paralysis of the deltoid, a flicker of movement in biceps and grasp reflex was normal before discharge at 36 days some shoulder movement was returning and at three months the left arm was considered to be normal. At the time we considered that this Erb’s palsy was probably due to pressure from the collar of the head box but did consider the suggestion that it was related to infection but there is no evidence of infection around that area and X-rays of the neck were normal.
A report an example of monoparesis as a complication of continuous positive airways pressure with a head box (figure). A male infant birth weight 2190 G at 35 weeks gestation developed respiratory distress syndrome at 34 hours. He was placed in a Vickers head box with maintained pressure of 10 cm. A “head box” is used for babies who can breathe on their own but still need extra oxygen. A hood is a plastic dome or box with warm, moist oxygen inside. He remained in the box gradually improving until the six days when his progress was complicated with staphylococcal septicaemia. With antibiotics he slowly improved and as he was becoming more vigorous by the 12th day abnormality of the left arm was noticed there was a complete paralysis of the deltoid, a flicker of movement in biceps and grasp reflex was normal before discharge at 36 days some shoulder movement was returning and at three months the left arm was considered to be normal. At the time we considered that this Erb’s palsy was probably due to pressure from the collar of the head box but did consider the suggestion that it was related to infection but there is no evidence of infection around that area and X-rays of the neck were normal.
This was the third report of such a complication.
This report was from St Mary’s Maternity Hospital Leeds where I was responsible for neonatal care of 3000 babies per year!
Dr David Eastham was a general practitioner (family doctor) who had sessions there helping me with the neonates; the obstetric senior house officers also helped out.
Doreen Burton was the excellent Sister in charge of the Special Care Unit. When the maternity and the neonatal units moved to St James’s in 1980, Doreen took over the larger combined neonatal unit there.
Ghosh SK. Littlewood JM. The clinical picture of coexisting toxoplasma and toxocara infection and its management. A small child with a rare double infection. [ Case Reports. Journal Article] Clinical Pediatrics. 15(1):31-3, 1976 Jan. pubmed.ncbi.nlm.nih.gov/1245080/
Dr Salil Ghosh was the senior registrar in Infectious Diseases at Seacroft Hospital, Leeds. We reported a boy with positive diagnostic criteria for both Toxocara infection (visceral larva migrant) and active Toxoplasma infection. Apparently the only case report of its kind at the time
Toxocariasis is an illness of humans caused by larvae (immature worms) of either the dog roundworm (Toxocara canis), the cat roundworm (Toxocara cati) or the fox roundworm (Toxocara canis).
Toxoplasmosis is a disease that results from infection with the Toxoplasma gondii parasite, one of the world’s most common parasites. Infection usually occurs by eating undercooked contaminated meat, exposure from infected cat feces, or mother-to-child transmission during pregnancy.
We reported a 3 year old Sikh boy had a two month history of irregular fever, malaise, lethargy. He had hepato-splenomegaly of 2 cms and generalised lymphadenopathy. He had extensive investigations which showed hypergammaglobulinaemia, anaemia and a Toxocara fluorescent antibody test positive 1:256 IgG and 1:16 IgM. The Toxoplasma dye test positive 1:16,000 and the titre of fluorescent Toxoplasma IGM1:1,1024. He gradually improved on 4 weeks pyrimethamine and sulphadiazine and was well when seen at 2 months.
We had help from Professor Alan Woodruff (1916-1992) of the Hospital for Tropical Diseases London, an international expert on tropical diseases, and Dr Donald H Garrow a distinguished consultant paediatrician at Amersham and High Wycombe from 1962-83 who performed the toxocara antibody tests. Both these doctors provided helpful criticisms.
Littlewood JM. Lee MR. Meadow SR. Treatment of childhood Bartter’s syndrome with indomethacin. [ Case Reports. Letter] Lancet. 2(7989):795, 1976 Oct 9. pubmed.ncbi.nlm.nih.gov/61458/
A letter with a brief first report of our patient with Bartter’s syndrome treated successfully and safely with indomethacin in response to a letter suggesting their safety has not been established in children.
The full report published in 1978 follows below.
Littlewood JM. Lee MR. Meadow SR. Treatment of Bartter’s syndrome in early childhood with prostaglandin synthetase inhibitors. [ Case Reports. Journal Article] Archives of Disease in Childhood. 53(1):43-8, 1978 Jan. pubmed.ncbi.nlm.nih.gov/415668/

The patient presented at the age of 9 months because of poor weight progress. He weighed 6.75 kg (1kg below the third centile) and was 70.5 cms long (50th centile). There was generalised wasting and hypotonia. cardiovascular system was normal with a blood pressure of 100/55. The plasma potassium was 2.4, sodium 131, bicarbonate 131 and urea 4.8 mmol/l, Intravenous pyelogram revealed large but otherwise normal kidneys. An ECG showed changes compatible with mild hypokalaemia.Plasma renin was very high but the plasma aldosterone was less strikingly raised.
The figure shows an infant with Pseudo-Bartter’s Syndrome secondary to electrolyte losses in cystic fibrosis but the appearance is identical to the present infant on presentation. Cheerful but very thin.
 Treatment was started at 11 months by increasing the intake of potassium to total of 80mmol/day which caused transient weight gain but no change in plasma potassium levels. On the advice of Dr Frederic Bartter (known to Dr Lee) spironolactone 18.75 mg/day was added at 11 months and although the plasma potassium rose to normal there was no effect on his poor growth and weight gain. At 28 months sodium intake was increased by adding 3g sodium chloride /day after which there was a definite increase in activity but no improvement in his weight.
Treatment was started at 11 months by increasing the intake of potassium to total of 80mmol/day which caused transient weight gain but no change in plasma potassium levels. On the advice of Dr Frederic Bartter (known to Dr Lee) spironolactone 18.75 mg/day was added at 11 months and although the plasma potassium rose to normal there was no effect on his poor growth and weight gain. At 28 months sodium intake was increased by adding 3g sodium chloride /day after which there was a definite increase in activity but no improvement in his weight.
At 33 months indomethacin was started at a dose of 2.5 mg three time daily, gradually increased to 20mg per day in divided doses over 4 weeks. The effect on growth and symptoms was dramatic. Within days the polyuria and thirst ceased and the constipation improved. There was a marked growth spurt which coincided exactly with the start of indomethacin (figure 1).
At 3yrs 9ms after 12 months indomethacin therapy was changed to ketoprofen 30mg daily with less risk of side effects than indomethacin. Within 4 days off treatment his thirst increased partially relieved by starting ketoprofen and completely controlled by increasing to 60mg daily over 6 weeks (figure 2).
The exact nature of the prostaglandin abnormality in Bartter’s syndrome remains controversial. Numerous investigations were carried out and are described in the paper and the many colleagues involved are mentioned in the acknowledgements.
Many people contributed to the investigation and management of this boy. We thank the parents (who were both doctors) for cooperation particularly during the demanding metabolic study; Sister Moriaty and the nursing staff of the outpatients at Seacroft Hospital; Dr M Dillon at the Hospital for Sick Children for initial plasma aldosterone and renin determinations; Dr S G Ball Dept of Medicine Leeds General Infirmary for later rennin determinations; Dr Frank Burnet, John Radcliffe Hospital Oxford for urinary prostaglandin measurements; Mrs M Cawood and Dr M J Levell, Leeds Suparegional Assay Service for later determinations of aldosterone; Dr L Birkinshaw, Dept of Medical Physics Leeds General Infirmary for total body potassium determinations; Mr Alan E Steel and Dr Angela Robinson for biochemical and haematological estimations; Mrs Susan Pattinson for dietary advice and my secretary Mrs Christine Silburn for secretarial assistance.


Michael Lee at the time of this publication was working in the General Infirmary. He later became professor of Clinical Pharmacology in Edinburgh and a Fellow of the Royal Society of Edinburgh. He maintained this was the most interesting patient of his career! He knew Fred Bartter and they discussed the problem.
Frederick C Bartter (1914-1983) was an American endocrinologist best known for his work on hormones affecting the kidney and his discovery of syndrome of inappropriate antidiuretic hormone and Bartter syndrome. Apparently he had a separate interest in mushroom poisoning.
Littlewood JM. Neonatal screening: the present position. [ Journal Article] Midwives Chronicle. 90(1072):91-3, 1977 May. pubmed.ncbi.nlm.nih.gov/586487/
In May 1976 I was invited to give the Mabel Liddiard Memorial lecture which was published the following year in the Midwives Chronicle. I think this invitation came through Miss Little the Matron at St Mary’s Maternity Hospital Bramley in Leeds. We had been screening meconium for cystic fibrosis there from 1975 and Miss Little took a great interest and was very supportive.

Mabel Liddiard was a distinguished midwife and prolific writer of many editions of both The Mothercraft Manuel and the British Red Cross Society Infant Welfare manual
In the lecture I discussed the increasing use of antenatal screening with amniocentesis mentioning prediction on haemolytic disease by Douglas “Tiger” Bevis (1919-1994) in 1952, determination of fetal sex by Fritz Fuchs and Povl Rlls in 1956 and chromosome studies in 1966 by Mark W Steele and W R Brag. More recently not only had a variety of metabolic disorders had been detected by examination of the amniotic fluid but major structural abnormalities, for example increased alpha-fetoprotein in spina bifida.
Routine physical examination of the infant by the midwife or the doctor may be considered as a screening procedure for the majority of infants examined appear and are quite healthy. A number of significant other anomalies may be detected on first examination some of which are not apparent on outward inspection. For example a cardiac murmur indicating congenital heart disease, displacement of the heartbeat suggesting intrathoracic abnormality, a cleft of the soft palate, congenital cataracts and glaucoma, congenital dislocation of the hip, the presence of a single umbilical artery present in 0.72% of infants of whom 17.5% have major congenital anomalies. The detection of some of these conditions in the pre-symptomatic stage is frequently of a great value
The current situation in 1976 was discussed regarding screening for congenital dislocation of the hip, metabolic disorders such as phenylketonuria introduced in 1962, galactosaemia and the value of a urine Clinitest in jaundiced infants. Hypothyroidism was not screened for at the time but we managed to get that introduced in our region. Cystic fibrosis BM Meconium Test was still not accepted as reliable or worthwhile by most paediatricians, including my two senior consultant colleagues in Leeds, but we carried on successfully screening with it.
I have always been keen on screening since carrying out my survey for neonatal urinary infections in the Sixties so I introduced screening for cystic fibrosis in East Leeds in 1975 when I was responsible for neonatal care at St Mary’s Maternity hospital – a world first! Or so I thought but the year before a distinguished Italian paediatrician, Professor Gianni Mastella, had started CF neonatal screening in Verona.


Director CF Trust
Eventually in 2001 Rosie Barnes and myself on behalf of the CF Trust, after a vigorous 5-year campaign, persuaded the then Health Minister, Yvette Cooper (who was pregnant at the time) to ignore the National Screening Committee’s misguided objections and introduce national neonatal screening for cystic fibrosis; by 2007 screening of all newborn infants throughout the UK had been introduced. This was one of our major victories at the CF Trust.
We were very fortunate in having these two experts involved.
Addendum. In hot weather infants with cystic fibrosis may develop a condition termed “Pseudo-Bartter’s syndrome”. The condition is related to excessive salt loss through sweating. The appearance before treatment is very similar to that of our patient when he first presented. In cystic fibrosis children simple salt supplements will correct the situation and prevent the problem.
Smith SE. Littlewood JM. The two-film barium meal in the exclusion of coeliac disease. [ Journal Article] Clinical Radiology. 28(6):629-34, 1977 Nov. pubmed.ncbi.nlm.nih.gov/589918/
The barium meal has a characteristic appearance in children with coeliac disease. This. study by Dr Sydney Smith was an attempt to document these changes. Our prospective experience over five years is described in assessing the two-film barium meal as a test for the exclusion of untreated celiac disease in children in order to try to make jejunal biopsy unnecessary.
287 meals were examined in children between 3 months and 10 years of age with a variety of gastro-intestinal symptoms and signs that might be attributed to celiac disease. From the two-film barium meal the calibre and transverse mucosal folds of the upper small bowel were measured.

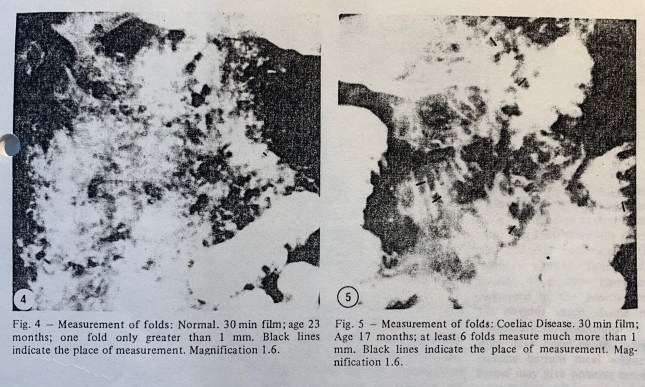
In 48 children with untreated coeliac disease there were only three (6%) with negative two-film barium meals. In 45 children with malabsorption from causes other than coeliac disease, there were four (9%) with negative two-film barium meals.
It is concluded that the two-film barium meal is a reasonably reliable test for the exclusion of untreated coeliac disease in children. It is simple, cheap, safe and economical of radiological time, and it compares favourably in accuracy with other screening tests, other than jejunal biopsy.
Sydney Smith was a senior consultant radiologist with a particular interest and expertise in paediatric radiology. He was very popular with paediatricians and his opinion greatly respected. He would always help and was very skilled in dealing with children. He was soon involved in our jejunal biopsy service in manipulating the biopsy capsule from the stomach into the duodenum. Also when our senior registrar John Davies was developing pancreatic function tests in children Sydney was essential is placing the special Hadorn triple lumen tube in the duodenum.
Sydney did so much for us paediatricians and our patients that I negotiated with the British Paediatric Association that, although not a paediatrician, he be invited to join – they agreed. But Sydney decided he didn’t want to join!!!!
Littlewood JM. Jacobs SI. Ramsden CH. Comparison between microscopical examination of unstained deposits of urine and quantitative culture. Archives of Disease in Childhood. 52(11):894-6, 1977 Nov. pubmed.ncbi.nlm.nih.gov/339849/
It had been our practice for some years to examine a urine for infection by microscopy of fresh unstained centrifuged deposit in addition to the standard bacteriological culture. This paper reports the relationship between this microscopical examination and the subsequent quantitative laboratory report. Examination of centrifuged deposits compared very well with subsequent culture results – 87% of infected urines were detected and only 6% of uninfected urines wrongly identified. There was less satisfactory correlation with uncentrifuged urine specimens.
So the results of this survey did support my belief that urinary infection could be identified by direct microscopy of unstained urine – preferably of a spun deposit.
Sister E Godfrey and her staff in St James’s paediatric outpatients meticulously collected all the samples. Although we did not move the paediatric wards from Seacroft to St James’s until 1980, I had busy sessions at St James’s during the Seventies where the nurses’ careful measuring and weighing of the children the years was central to my later observing the adverse effect of inhaled steroids on the growth of some asthmatic children (see 1988 Lancet letter)
Mr Colin Ramsden was a cheerful, helpful and very able a Senior Laboratory bacteriology technician at St James’s. He was involved with me in other studies in subsequent years including what I regard as the most important publication of my career on the early eradication of Pseudomonas aeruginosa in children with cystic fibrosis (Littlewood JM, Miller MG, Ghoneim At, Ramsden CH. Lancet 1985 Apr13;1(8433):865. PMD 2858721)
 Dr Sidney Jacobs (image from our 1956 degree photo) and I both qualified in 1956 at Leeds Medical School.
Dr Sidney Jacobs (image from our 1956 degree photo) and I both qualified in 1956 at Leeds Medical School.
Sid at the time of this study was consultant microbiologist at St James’s. He always maintained he preferred the laboratory to seeing patients in the clinic. So he first became a bacteriologist and then eventually an H. M. Corone
Ghosh SK. Littlewood JM. Goddard D. Steel AE. Stool microscopy in screening for steatorrhoea. [ Journal Article] Journal of Clinical Pathology. 30(8):749-53, 1977 Aug. FREE pubmed.ncbi.nlm.nih.gov/599187/
A prospective study is described comparing microscopy of random faecal specimens for the presence of neutral and split fat by a relatively simple, cheap, and rapid method with standard chemical estimation of faecal fat.The method of microscopy was found to be reliable in excluding steatorrhoea in children over the age of 3 month.
100 children 46 boys 54 girls aged between 11 days and 15 years from the paediatric infectious diseases departments of Seacroft hospital and the neonatal unit at St Mary’s hospital leads were included in the study. The specimen of faeces is thoroughly mixed with an application to stick and small amounts about 5mm in diameter placed on two microscope slides. For neutral fat two drops of water, 2 drops of 95% ethyl alcohol mixes in. One or two drops of a saturated solution of Sudan 111 in 95% alcohol is added with the edge of the cover slip which is then applied and the preparation examined under the microscope using a x400 lens.


For split fat several drops of 36% acetic acid are added to the specimen on the second slide followed by several drops of Sudan 111 and mixed with edge of the cover slip then gently heated over an alcohol burner and repeated three times before examination using the same lens.
 The results were graded into three groups (details in the full paper) and plotted against the biochemical findings.
The results were graded into three groups (details in the full paper) and plotted against the biochemical findings.
Apart from ease of collection of the sample other advantages of the microscopic assessment of faecal fat or economy of time it takes less than 10 minutes as opposed to 90 minutes for by chemical assessment because the material for the analysis signature negligible and this method is spreading the hazards of homogenisation of faecal matter which is undertaken during the assessed by chemical assessment.
We thanked Dr John Stevenson and Dr Bert Pullen of the consultants in the infectious disease department Seacroft for inclusion of their patients,; the sisters and staff of Seacroft Hospital and St Mary’s Hospital; Mr K Bramald of the Bacteriology Department for technical help; Dr G L Gibson Director of the Regional Public Health Laboratory at Seacroft for helpful advice; and last but not least my secretary Christine Silburn
Dr Salil K Ghosh was my senior registrar at the time – probably in his Thirties. I think he went to the General Hospital Middlesborough as consultant in Infectious Diseases. Writing this in 2020 I could not trace him presumably long retired and well into his Seventies.
Some years later we reassessed the method for use in children with cystic fibrosis where it also proved to be very useful. (Walters MP et al, 1990 summarised in the Nineties section)